by Brian Lipsett, PhD and the Environmental Background Information Center
for Public Interest Law Center of Philadelphia
This document may contain material which is protected by Attorney Client Privilege
Please Do Not Quote or Cite
July 14, 2000
The purpose of this analysis is to assist the Public Interest Law
Center of Philadelfor phia in developing a comparative public health based
criteria advancing Environmental Justice. In general we were concerned
with the census tract mapping of four health factors in Philadelphia,Pa.(1,500,000
pop., 367 census tracts).
* Age-adjusted cancer mortality rate
* Age-Adjusted non-cancer mortality rate
* Infant mortality rate
* Low birth weight rate
Additionally, the Environmental Background Information
Center (EBIC) was concerned with the spatial analysis of human population
data in
Pennsylvania and its relation to the existing sources of environmental
stress such as solid waste and hazardous waste treatment nod disposal facilities
as well as
manufacturing facilities and coal mining facilities.
The rationale for the public health study is based on the view that a community that has substantially worse public health than the median (or average) public health of the population in the other areas of the city or county or state, should not have its poor public health exacerbated by the introduction of a new source of environmental stressors.
The public health study, it should be noted, concerns the existing community health regardless of the possible causes of the condition; the study does not examine the environmental conditions or the effects of odors, noise, mobile emissions, psychological conditions or personal habits, or cultural habits, or educational levels, or income levels, or medical facilities, etc., all of which certainly affect individual health and community public health.
This is not to say that there may not be strong correlations
between the public health of a community and one or more of the above noted
conditions. The EBIC study was designed to examine how human health
factors were distributed spatially with respect to environmental risks
and other demographic features of the
population.
To undertake this study we used a number of statistical
tools to help explore and explain these relationships. in the opening section.
In the opening section, I address this problem at a level of abstraction
which is specifically intended to provoke the reader. Immediately this
provocation is likely to lead the reader to dismiss the text insofar as
it belabors the obvious. However this might arise, the challenge I present
here to the reader is to provoke thought which pushes the human condition
to a level of abstract consideration which sets aside blame and guilt for
purposes of a more general consideration of the circumstances which we
all arbitrarily find ourselves in after we are born and become conscious
of our material status.
Summary of Key Preliminary Findings
Our work with numerous datasets made available from state and federal
agencies informs us that at the municipal level in PA:
Research on human population distribution is certainly not new. However,
research on human population distribution which examines the distribution
of social resources is emerging as a relatively new and increasingly sophisticated
field. Some research along these lines has shown evidence of racial and
class discrimination, for example, in the amount of environmental risk
to which human populations are exposed. Environmental risk constitutes
a form of negative social resource which, in some research, has come to
serve as an indicator of broader social discrimination. In our view, this
type of research represents an advance in our current means of understanding
the social structure which we all inhabit. While it is far from a perfect
research regime, it offers considerable insight into the manner in which
we perceive, experience and share our own environment in our own communities.
In this section, I outline a broad view of the approach to this research
project.
The relative geographic distribution of different age, class, racial
and ethnic sub-populations across space is an institutional dimension of
modern society. By institutional, I mean that the circumstances of different
groups (racial and class groups in particular) largely exist prior to our
own individual existence and perception. Within this context, there is
a close relationship between the distribution of human population groups
and human activities such as waste handling, manufacturing, and mining.
These phenomenon coincide with certain geographic/natural features of land.
Features which make - and have made - certain areas more desirable for
purposes of human occupation, settlement, and economic activity.
Human population distribution is thus the result of a convergence of
numerous factors including geologic and historical processes, cultural,
familial, and physical proximity and the availability of a livelihood of
some sort. Some places are better for human habitation because, for various
reasons, they are more habitable. Some places, while not more habitable
than others - perhaps even less so - support large populations because
of the emergence of significant economic activity related to the flow of
goods and commerce - largely as the result of geographic features beneficial
to human trade such as transportation infrastructure.
At issue in environmental justice research is whether or not such geographically
located sub-populations are a) disadvantaged and b) exposed to serious
risks from productive human activity for which no net benefits accrue which
might otherwise tend to ameliorate the conditions associated with being
disadvantaged, and c) caught in those conditions as the result of broader
patterns of discrimination stemming from systemic racism. In this analysis,
I attempt to discern some of the patterns associated with the hypothesis
that class and racial discrimination is apparent in the distribution of
poor health and environmental risk.
Literature
A considerable body of literature has emerged on the topic of environmental
justice. Only a small portion of it is empirical and that portion is somewhat
varied in its findings. This variation in analytical results can be summarized
as arising from different research methodologies (see Lipsett and Mennis,
1999). In particular, these research methodologies vary in their approaches
temporally, in scope, and in scale. Temporal variation in analytical
results is related to the chicken and egg question: i.e. do disadvantaged
groups move into areas where environmental risks already exist or do the
risks move into areas where disadvantaged groups already live? Methodologies
which approach this question have come up with varied results, but they
are relatively rare and many feel the question is, for all intents and
purposes, irrelevant. Temporal analyses are largely limited in scope
to certain confined geographic areas rather than an entire region or the
entire nation. Still other variation in results arise out of methodological
variation related to the scale of the analysis. This matter is also
referred to as the "resolution problem:" i.e. What is the appropriate geographic
unit to which population data should be aggregated for purposes of analysis?
Many studies focus on this matter and follow a narrow track, arguing for
the appropriateness of one or another geographic unit for purposes of analysis.
A different literature addresses the spatial clustering of human health
problems, in particular, various types of cancer and their occurrence around
sources of pollution (e.g. toxic dump sites, manufacturers, etc). Some
studies have established statistically significant relationships between
sources of pollution and human health problems, but most studies do not,
usually because of relatively small sample sizes. However, a small body
of literature has examined such things as respiratory mortality and air
quality and found statistically significant relationships. For a number
of reasons including lack of resources and a lack of sensitivity in the
structure of the data available to us, this analysis does not attempt to
establish such relationships. Rather
we are simply seeking to identify and characterize communities with substandard
health and/or contain environmentally hazardous facilities.
Data
This analysis is derived
from data which was obtained from a number of different sources including
the Philadelphia Department of Health, the Pennsylvania Department of Public
Health, the United States Department of Health and Human Services Center
for Health Statistics, the United States Envheironmental Protection Agency,
the United States Department of the Census, the Pennsylvania Department
of Environmental Protection and others. We obtained statistical health
data for four health outcomes in Pennsylvania and Philadelphia; Total Mortality,
Cancer Mortality, Infant Mortality, and Low Birth Weight. These data were
averaged over five years - 1992 to1996. These statistics were derived from
data provided by the Pennsylvania Department of Public Health for each
municipality and county in Pennsylvania and the Philadelphia Department
of Health for census tracts in Philadelphia. The health data was combined
with demographic data from the 1990 U.S. census as well as population projections
for 1996, 2001 and 2006 provided by the Environmental Systems Research
Institute (ESRI). We also obtained and examined data on manufacturing activity,
solid waste and hazardous waste disposal activity, and coal mining activity
from the U.S. EPA's TRI, RCRIS, and BRS databases and the Pennsylvania
Department of Environmental Protection.
Methodology
This paper addresses the
problem of the spatial distribution of human health, demographic and environmental
risk phenomenon through a limited multi-scalar analysis which is confined
in scope to the state of Pennsylvania. The overall approach taken here
is to utilize three scales of resolution, the county, the municipality,
and the census tract. In addition, statewide levels are applied as an additional
background standard. It should be noted here however, that health data
in Pennsylvania is collected by the state at the municipal level and is
coded so that it can be aggregated to the county level. In Pittsburgh and
Philadelphia, human health data is also aggregated at the census tract
level, allowing for an additional scale of detail for those areas. This
"data reality" does have a limiting effect on our analysis, however I believe
that the multi-scalar approach taken here mitigates some of the problems
noted in the literature, at least somewhat.
Our statistics were standardized
to derive rates for respective geographic units; i.e. census tracts, municipalities
and counties (note; at this stage this discussion only applies to the state,
county and municipal levels and not for Allegheny and Philadelphia County
census tracts). Cancer mortality and total mortality data was age adjusted
to account for variation in age groups between various municipal levels.
The age adjustment standard we utilized is the 1940 standard million. The
health data was combined with demographic data from the 1990 U.S. census
and we then added data on manufacturing activity and hazardous waste disposal
from the U.S. EPA's TRI, RCRIS, and BRS databases. These different datasets
were combined through spatial and code specific techniques to generate
files which incorporated all relevant data which applied to each of the
geographic units in question.
Subsequent to mapping relevant
data, we conducted a number of statistical analysis of the data to determine
the apparent relationships between the environmental, demographic, and
health data characteristics of each spatial unit (i.e. county, municipality,
census tract). Because of the data structure and functionality of GIS databases,
it is relatively easy to conduct statistical analysis of data for purposes
of understanding the relationships between various characteristics of geographic
units (counties, municipalities). More advanced statistical techniques
also allow the analysis of the spatial relationship of various health and
demographic characteristics of and between various geographic units. Because
there is considerable variation in the size of the geographic unit in our
analysis, the minor civil division, we controlled for the size of the region
by including its area and the number of people, families and households
in the region in the regression analysis. Our findings are discussed in
more detail below.
In Philadelphia, we also
standardized the data by ranking census tracts in terms of the four health
outcomes we acquired from the city (infant mortality, cancer mortality,
total mortality and low birth weight rates). In addition, we generated
two additional health outcome categories which were useful: non cancer
mortality and overall health. Non cancer mortality was derived by subtracting
the age adjusted cancer mortality rate from the age adjusted total death
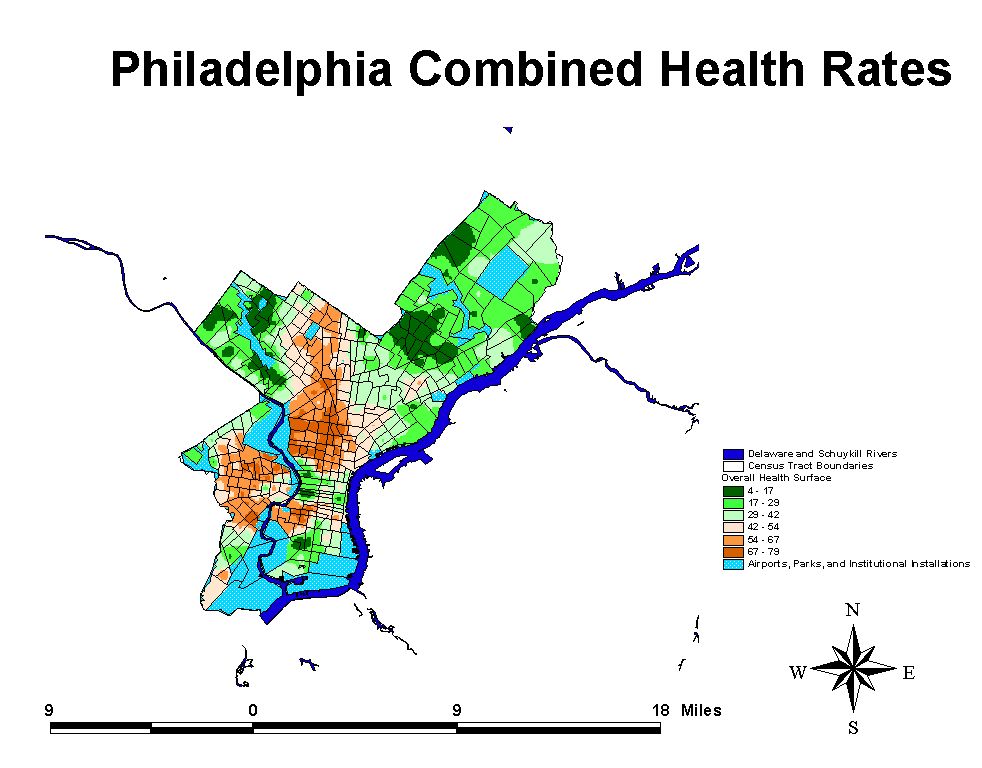
rate. Overall health rates were derived by breaking the population into
20 different groups of 5% based on each rate of health outcome. These percentile
groups were coded one to twenty with twenty being applied to census tracts
with the poorest health for each outcome. I then added the percentile codes
for cancer, non cancer, low birth weight rate and infant mortality together
and ranking the resulting scores (4 for best combined health to 80 for
worst combined health) by the same percentile ranking system (1 - 2O).
The overall health variable is useful because it helped to identify areas
where people are being hammered with a combination of all poor health outcomes.
The approach taken utilizes
several different analytical techniques which are based on Geographic Information
Systems as well as statistical and spatial statistical analyses. Age adjustment
of the total and cancer mortality rates for each municipality was accomplished
with software provided by the Centers for Disease Control. Several different
software packages aided us in this analysis including ArcView, ArcView
Spatial Analysis Extension, SPSS, Splus, Splus Extension for ArcView, SPlus
Spatial Statistics, and Health Information Retrieval System.
Findings
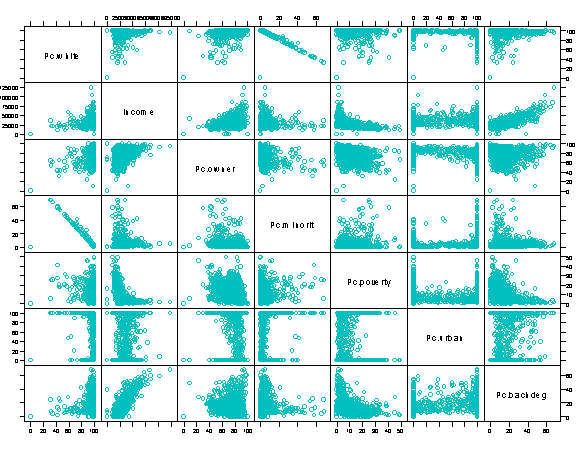
The first section of findings discusses some overall general bivariate relationships apparent in the Pennsylvania data. Each following section discusses a number of complex mulltivariate relationships which help us to get a sense of the structure of the social order in PA and, to a lesser degree, the factors affecting the health of Pennsylvanians in terms of four particular outcomes - infant low birth weight and mortality rates, cancer and total mortality rates. The initial section begins with an overview of the relationships of some of the data in the research model. A number of variables reveal fairly intuitive relationships. Percent Minority and Percent White for example are inversely correlated although not entirely collinear because of variation in the percentages of percent white hispanic between municipalities.
Click
on the Graph to see a Larger Version
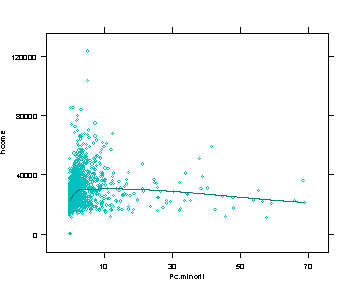
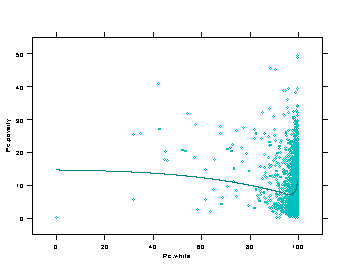
Similar correlations exist between percent bachelor's degree and income. As the percentage of people with a bachelor's degree or higher increases, the median municipal household income increases. As the income level increases, the percentage of people owning homes increases. These more or less intuitive relationships aside, there are other less obvious bivariate relationships which are apparent in the data. For example, as percent minority increases, income levels increase until about 5% minority. The regression line levels out dropping slightly to about 30% minority, which is slightlyhigher than the 24% overall minority level in the United States Census figures from the entire nation. After 33% minority, income levels begin to fall more rapidly. This relationship, not surprisingly, is the mirror image of the relationship between income and percent white, once again illustrating that high poverty rates tend to occur in highly segregated communities more frequently than in integrated ones, although it must be stressed that the very highest income municipalities in Pennsylvania tend to be predominantly white.
In other words, income levels
in Pennsylvania are low in certain types of communities which are predominantly
white, and other communities which are predominantly minority. This particular
reality is best understood in terms of the nature of community structure
in Pennsylvania. Impoverished minority populations tend to be clustered
in a small number of larger urban municipalities whilst high concentrations
of impoverished white people tend to be scattered in rural areas in Pennsylvania.
67.5% of all municipalities in Pennsylvania are classified as 100% rural.
22.8% are classified as 100% urban. The remaining .7% of all municipalities
fall somewhere in between those extremes. Thirty-nine municipalities in
PA (1.5%) contain populations with greater than 24% minority, the national
background figure. 77% of those municipalities are greater than 50% urban.
84 PA municipalities (3.3%) contain minority populations greater than 12%,
the state background figure. Once again, 77% of those municipalities are
greater than 50% urban.
The degree to which this
apparent segregation is the result of systematic individual or institutionalized
racism probably can never be discerned. But it must be seen as a key factor.
To ignore it, or to suggest other explanations for the phenomenon belies
the point. Historical processes, geographic features, land use patterns,
proximity to transportation routes, all of these may in various ways contribute
to the phenomenon, but they do not dismiss the striking evidence of a segregated
society, as evinced in 1990 Pennsylvania population data. Having said that,
a key point which has been ignored is that racial segregation of communities
is one of a number of features of a discernable pattern of broad scale
social injustice.
Poverty in rural white communities
in Pennsylvania is also marked, and evidence of environmental injustice
arises in these communities as well. To emphasize the point, bear in mind
that when communities in PA have high percentages of whites, the poverty
rate tends to increase sharply, to levels almost (but not quite) as high
as those of municipalities with high percentages of minorities. Granted
that there are some extremely wealthy, low poverty communities which are
predominantly white but they are not the only type of white community and
they are not the rule.
Multivariate Analysis
Up till now, of course we've
been talking about relationships which are strictly bivariate and do not
control for the impact of other factors. These more complex relationships
can be better understood using multi-variate techniques a matter to which
we now turn. Because there is considerable variation in the size of the
geographic unit in our analysis, the minor civil division, we controlled
for the size of the region by including its area and the number of people,
families and households in the region in the regression analysis. The models
and all results, unless otherwise characterized, are statistically significant
at the .05 level or greater.
Poverty
The relationship between
various demographic, and environmental factors and poverty rates in political
units in Pennsylvania shows that poverty rates are dependant on a number
of factors. Not surprisingly, as median household income levels increase,
poverty levels decrease. Educational variables appear in this model to
have a counterintuitive effect on poverty rates. As the percentage of people
with advanced educations increases, poverty levels increase. Lastly, as
the percentage of minority status individuals increases, poverty rates
increase. These data do not provide evidence that the presence (or absence)
of manufacturing, solid waste and hazardous waste disposal facilities have
any relationship with poverty rates at the municipal level. To generalize
these results, poverty rates appear to be influenced by a number of factors
but not the presence or absence of environmentally hazardous manufacturing
and hazardous waste disposal facilities. These findings suggest that the
"benefits" of environmentally hazardous facilities and poverty programs
do not appear to be reaching many segments of the Pennsylvania population.
Education
Educational attainment is
often viewed as an important factor in quality of life. Equally, access
to advanced education is another aspect of social inequality, with disadvantaged
groups having less opportunities for advancement. In this analysis, we
found that median household income had a considerable impact on educational
attainment. As income increases, educational attainment increases. Curiously,
as poverty rates increase, educational attainment also increases but only
incrementally. The percent minority and number of environmentally hazardous
facilities in a community had small negative effects on educational attainment.
Home ownership and percent rural all had negative impacts on educational
attainment. These results are somewhat counterintuitive but seem to point
to the importance of rural vs urban population settings and economic inequality
as defining features regulating educational attainment.
Race
Minority status is treated
as a dependent variable here in order to determine what factors are bound
up with that community feature at the municipal level. These results tell
us that as the percentages of homeowners increases, the percentage of minority
people in the municipality decreases. As the median household income goes
up, the percentage of minority people increases. This is also true for
poverty rates. As poverty rates increase, percent minority increases. Once
again, these results point to disparities in the structure of municipalities
with higher percentages of minorities and also clearly points out the fact
that most rural municipalities in the state tend to have high percentages
of whites.
Presence of Manufacturing
Facilities and their Releases
The presence of manufacturing
facilities poses a risk to communities when those facilities are known
to handle and release toxic chemicals. The magnitude of the risk to the
community, while the subject of an unrelenting debate, is not simply the
presence of a given facility in a community, nor the relative proximity
of human populations to such facilities. But also to the magnitude of the
releases, their relative toxicity, the medium to which they are released
and the proximity of people to potential contact with the release either
directly or in diluted form. Facilities releasing a class of over 650 chemicals
in amounts greater than 25,000 pounds are required to report those releases
to the federal government through SARA Title III of the Superfund or CERCLA
law. In this analysis we utilized TRI data reported for 1995 to test for
the relationship between this source of pollution and the composition of
communities containing them.
Our results indicate that,
in terms of the number of manufacturing facilities present in a municipality,
as the percentages of home ownership and percentage of people with bachelors
degrees goes up, the number of TRI facilities goes down. Conversely, as
the percentage of minority residents and the percent urban increased, the
number of TRI facilities increases. In terms of total releases to the environment,
a variable which is dependant on the number of manufacturing facilities
in an area, as the percentage minority increases, the level of emissions
into the environment also increases. These results indicate that manufacturing
facilities in Pennsylvania are typically clustered in communities with
high percentages of minorities who may be exposed to the emissions from
manufacturing activity. It also indicates that communities with larger
numbers of manufacturing facilities have lower educational attainment and
home ownership rates.
Presence
of Waste Disposal Facilities
TSDF facilities are facilities
which hold permits from the U.S. Environmental Protection Agency to handle,
treat, store and/or dispose of hazardous waste. Commercial TSDF's constitute
a smaller class of these facilities which are licensed to handle wastes
and take them in from other non-related business entities for a fee. Several
studies have shown that commercial TSDF facilities are most often located
in certain areas (zip code regions and census tracts) with higher percentages
of minorities than other non-TSDF containing areas (CRJ 1987, 1994, Been,
199x). One set of studies have disputed this relationship but only by eliminating
from the analysis all the populations in all census tracts in non-TSDF
containing MSA's and rural counties. Our research utilized data provided
by Been for commercial TSDF facilities. For a number of reasons, we felt
that such a list represented an incomplete inventory of waste disposal
activities so we added solid waste disposal facilities including sewage
treatment, solid waste transfer stations, landfills, and trash incinerators,
provided by the state of Pennsylvania to our analysis. We found that municipalities
with higher percentages of minority persons, and persons living in poverty
had larger numbers of waste disposal operations. Conversely, communities
with higher percentages of home ownership had fewer waste disposal facilities.
Presence of Manufacturing
and Waste Disposal Facilities
We further profiled the structure
of communities to determine what demographic characteristics determined
increased numbers of combined waste disposal and manufacturing sources
of environmental risk. Educational attainment, home ownership, and percent
rural had negative impacts on the total number of environmentally hazardous
facilities in Pennsylvania municipalities. Income and minority status have
linearly positive relationships with the number of environmentally hazardous
facilities. Although the mechanisms behind these former relationships are
unclear, it is suggested here that, once again, these findings are an indication
of operative disparities in municipalities with larger numbers of environmentally
hazardous facilities.
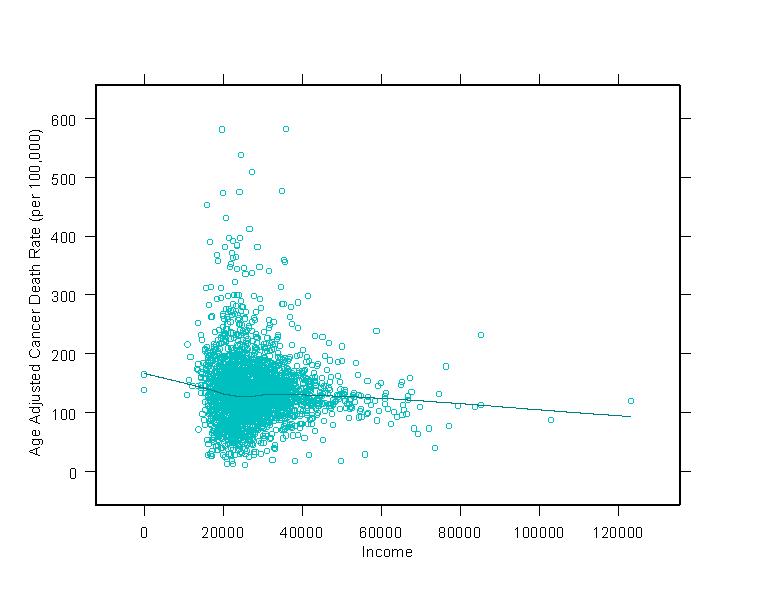
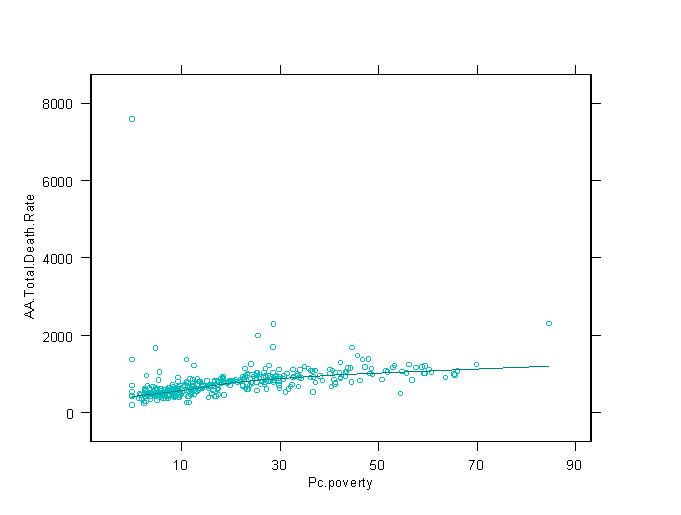
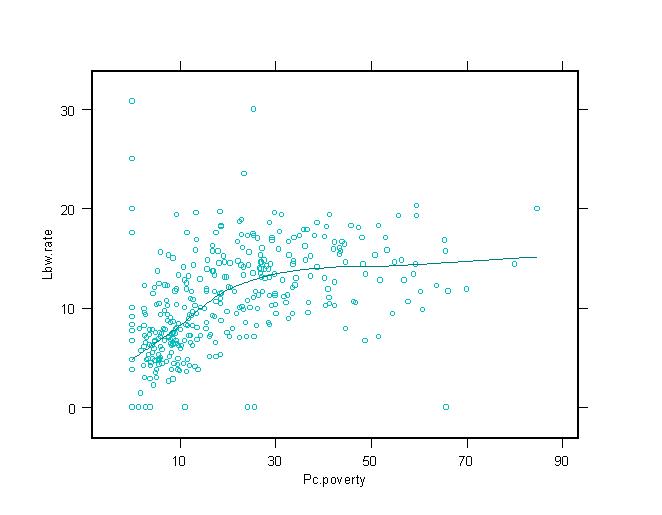
Human Health Outcomes
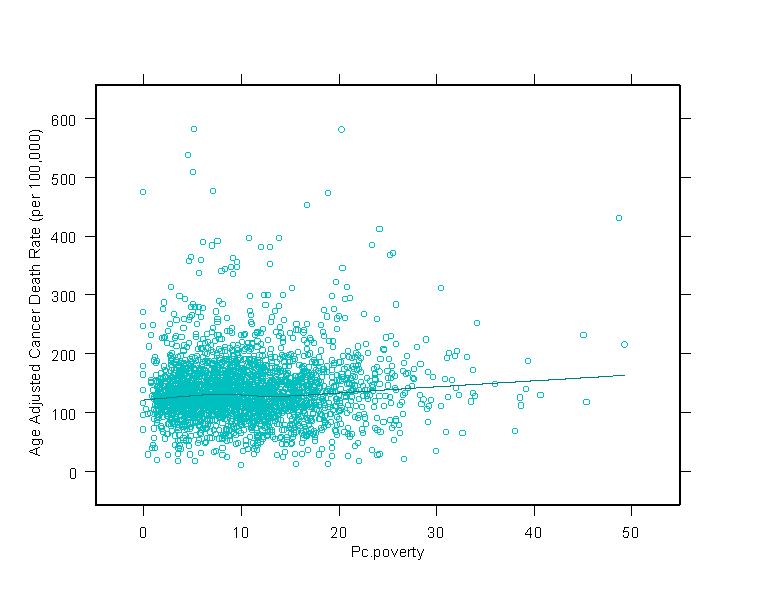
Health wise, there are some observable relationships that bear scrutiny. Poverty
and other indicators of diminished economic standing have long been associated
with poor health outcomes. This relationship is observable in these data. Age
Adjusted Cancer Mortality Rates, Age Adjusted Total Mortality Rates, Low Birth
Weight Rates, and Infant Mortality Rates are positively related to poverty rates.
As the percentage of people in municipalities living in poverty goes up, rates
for these health outcomes also go up. Poor people are, across the board, are more
likely to die earlier than people in better economic conditions. Income is, not
surprisingly, inversely related to these negative health outcomes. As median household
income goes up, mortality and low birth weight rates tend to go down. Some of
these relationships are illustrated in the graphs at right. In general economic
variables tend to have a positive relationship with health outcomes. As people
become more prosperous, their health gets better. Overall, national research indicates
that these economic variables drive human health and these findings are supported
in our
results in Pennsylvania. Multivariate
techniques such as those we use below are a bit less powerful than those above
involving demographics, manufacturing and waste disposal. However, there do
provide some insight that we discuss below.
Total Mortality
Total Age Adjusted Mortality
figures were derived from state municipal health data for the years 1992-1996
and standardized. 1990 ages for 18 age categories were utilized to age
adjust raw rates. The age adjusted figures were then plugged into a regression
model to derive statistical analysis of the demographic factors affecting
the health outcome. Our analysis tells us that home ownership and educational
attainment were negatively related to age adjusted total mortality rates.
Minority status, percent rural, and percent poverty were all positively
related to total mortality. These relationships speak to potential impacts
that are occurring within inner city and rural areas and impacting on poor
people, leading to elevated total mortality rates.
Cancer Mortality
In this model only two variables
appear to have any significant relationship to age adjusted cancer mortality;
home ownership and educational attainment. Both those relationships are
negative. This model is relatively weak insofar as it only accounts for
about 3.5% of the variation in the dependant variable.
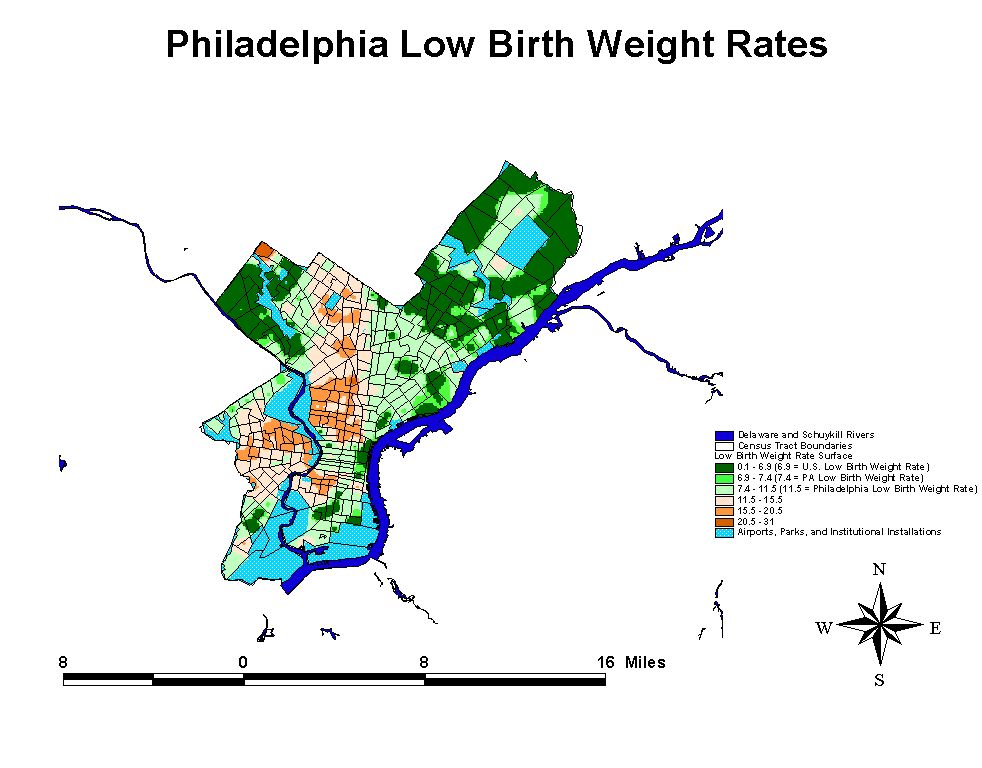
Low Birth Weight
In this model percent minority
is the only variable with a significant relationship to low birth weight
rates. This relationship is positive. Income is negatively related to low
birth weight rates. A considerable body of research involving elevated
low birth weight rates for minority populations has linked those outcomes
to a lack of prenatal care - a phenomenon which should also be correlated
with high poverty and/or low income sot his analysis, to some extent, conforms
to broader national level and regional research projects.
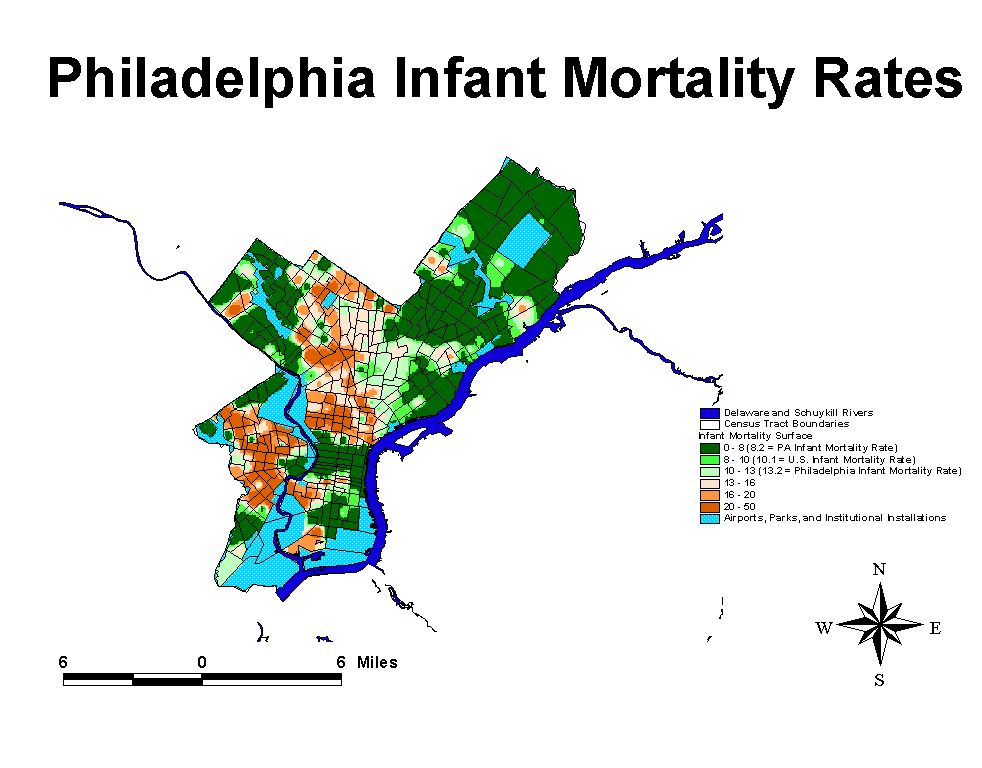
Infant Mortality
No statistically significant relationships were discovered between any
of the independent variables discussed above and infant mortality. However,
a considerable body of literature on this topic has linked infant mortality
to poverty and low income status.

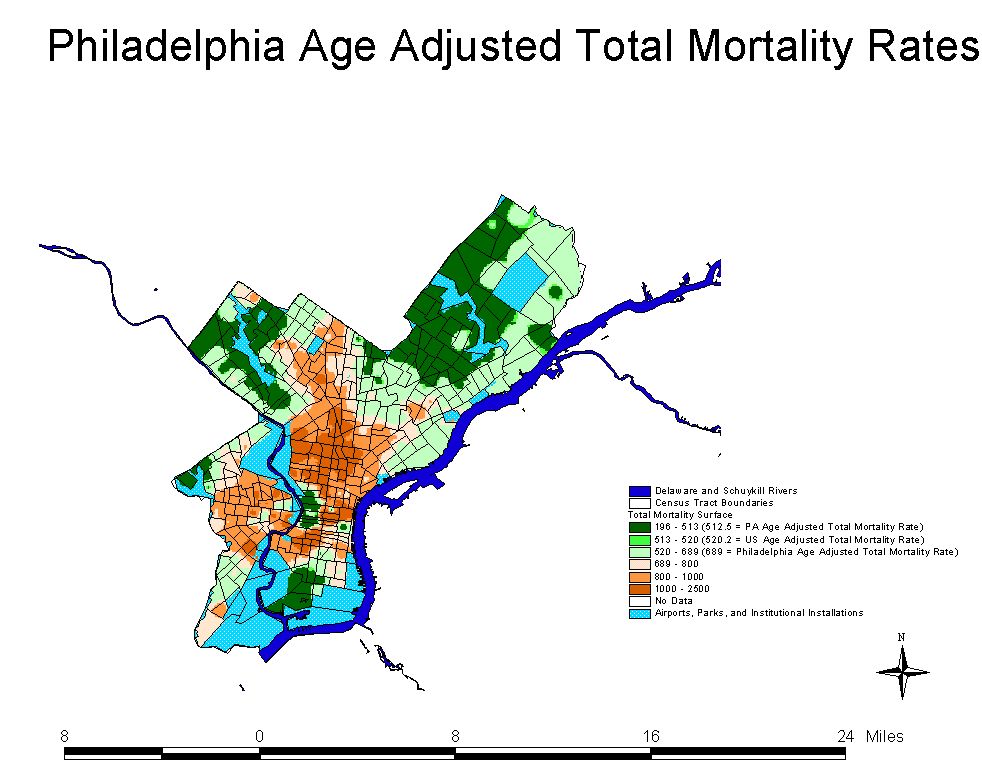
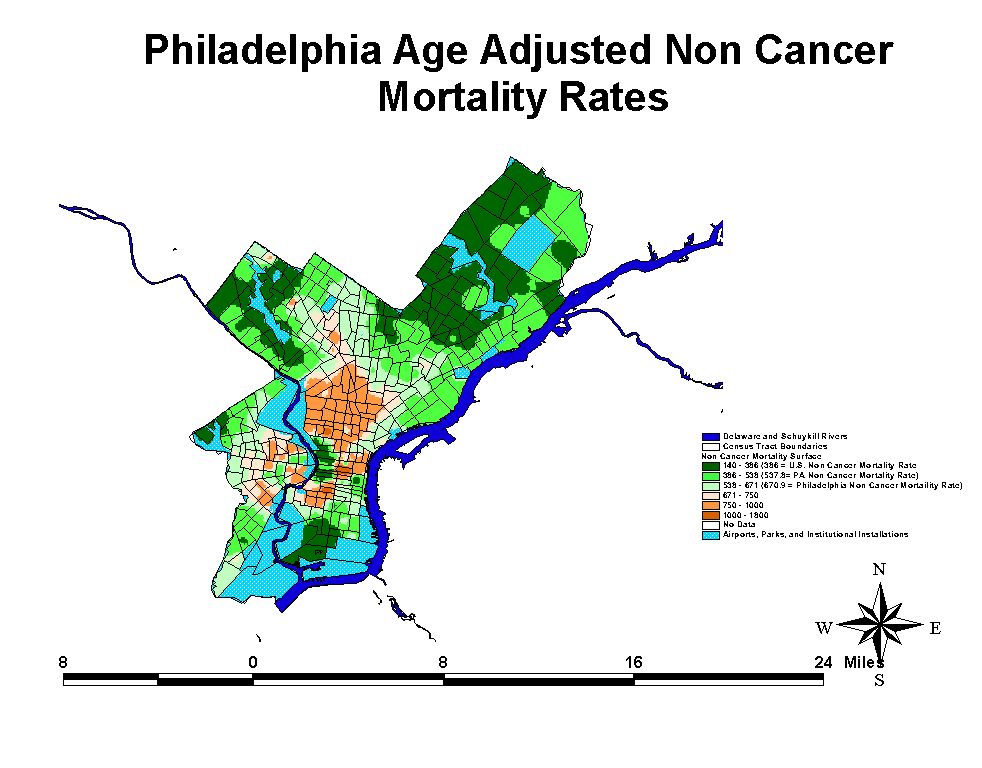
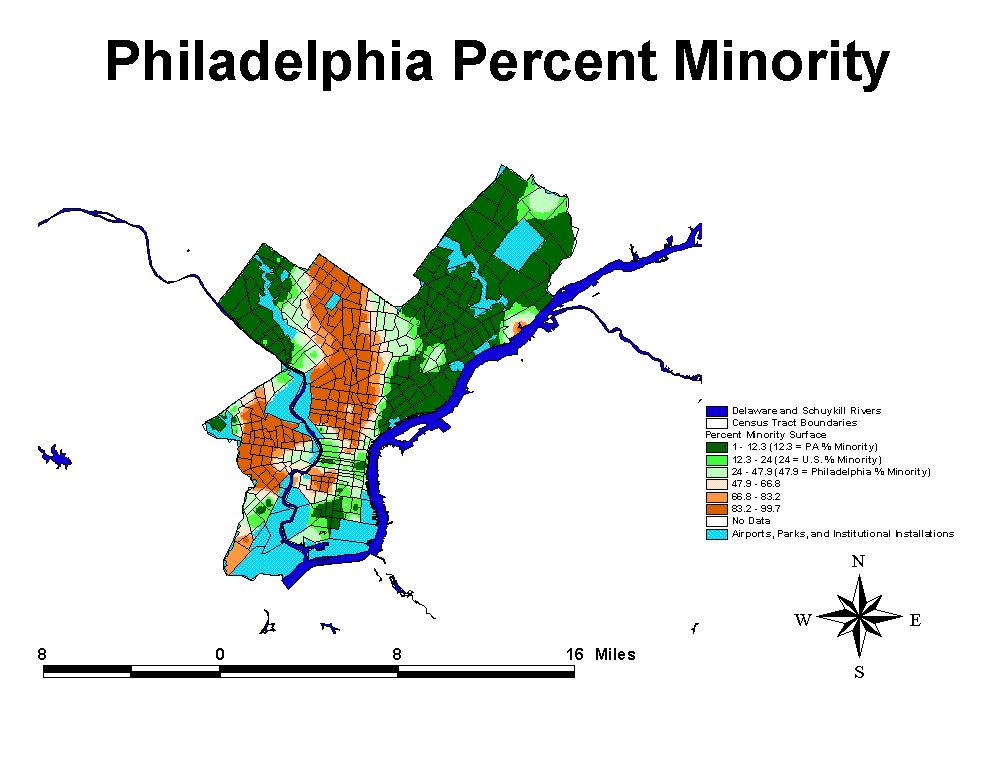
Health in Philadelphia Census Tracts
Philadelphia is not a very healthy
city with some of the highest rates of infant mortality, total mortality, cancer
mortality and low birth weight babies in the entire state. Not surprisingly,
within the city itself, there are even higher rates than the overall citywide
rate. This can be shown to be true because the city of Philadelphia collects
health outcome data at the census tract level.
Analysis of health and demographic data at the census tract level in Philadelphia
yields interesting bivariate results, but multi-variate regression techniques
utilizing the same basic model as used above, do not appear to be very helpful.
The reasons for this are unclear but may be due to outlying data. However, the
failure of the regression model to convey explanatory power at multiple scales
of geographic aggregation does not undercut the descriptive power of the readily
apparent bivariate relationships in the data. Here it should be noted that the
overall health of Philadelphia is poor, with poor health outcomes at elevated
levels compared to county and municipal averages. The census tract data indicate
quite clearly that the distribution of poor health in Philadelphia is not uniform,
conforming to the results of the above analysis. In short, some areas of Philadelphia
are experiencing poor health at a level which is far above
most municipalities in the state. As it turns out, those areas with poor health
also have elevated levels of poverty, lower incomes and more minorities. Conversely,
census tracts with good overall health are predominantly white, have higher
incomes, and lower poverty.
Descriptive statistics say much in this regard. By breaking the population down into 20 roughly equal groups, it can be shown that within the 20% of the Philadelphia population with the highest rates of poor overall health in terms of high rates of low birth weight babies, infant mortality, non-cancer and cancer mortality, 94.8% are minorities, 33.4% are living in poverty. This 20% of the population has an average household income of $23,230 per year. Of the 20% of the Philadelphia Population with the lowest rates for these health indicators, 8.1% are minority, 7.4% are living in poverty. The average household income for this group is $41,790 per year.
These same relationships hold true,
although in slightly lower magnitude in some cases, for all of the other variables.
Here it should be noted that Philadelphia is the most densely populated county
and city in the state and so it is something of an anomaly. However, a substantial
portion of the state's population is affected by these rates.
DiscussionThe core health problems affecting residents of the state are correlated in these data to low income, poverty, and low educational attainment.
Appendix I: Maps
and Graphs
Click on
the Map or Graph to see a Larger Version




Poverty
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 25.512 | .784 | 32.547 | .000 | |
| PERSONS | 1.039E-03 | .000 | 5.129 | 7.608 | .000 | |
| FAMILIES | -2.753E-03 | .000 | -3.253 | -6.534 | .000 | |
| HOUSEHOLDS | -1.005E-03 | .000 | -1.897 | -3.402 | .001 | |
| AREALAND | 2.165E-02 | .006 | .062 | 3.642 | .000 | |
| INCOME | -5.122E-04 | .000 | -.723 | -27.580 | .000 | |
| PC_OWNER | -3.948E-02 | .012 | -.068 | -3.361 | .001 | |
| PC_MINORIT | .166 | .019 | .138 | 8.508 | .000 | |
| PC_RURAL | 7.492E-03 | .003 | .049 | 2.471 | .014 | |
| TOTAL_NUMB | 5.326E-02 | .100 | .013 | .534 | .593 | |
| PC_BACHDEG | .114 | .018 | .155 | 6.168 | .000 |
a Dependent Variable: PC_POVERTY
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .679 | .461 | .459 | 4.874 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 52314.337 | 10 | 5231.434 | 220.261 | .000 |
| Residual | 61064.105 | 2571 | 23.751 | |||
| Total | 113378.443 | 2581 |
Education
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| (Constant) | 1.990 | .989 | 2.012 | .044 | ||
| PERSONS | -6.967E-04 | .000 | -2.520 | -4.768 | .000 | |
| FAMILIES | 5.500E-04 | .000 | .476 | 1.218 | .223 | |
| HOUSEHOLDS | 1.520E-03 | .000 | 2.103 | 4.853 | .000 | |
| AREALAND | 3.753E-03 | .006 | .008 | .592 | .554 | |
| INCOME | 8.262E-04 | .000 | .854 | 53.377 | .000 | |
| PC_OWNER | -.154 | .012 | -.194 | -12.657 | .000 | |
| PC_MINORIT | -7.567E-02 | .021 | -.046 | -3.610 | .000 | |
| PC_POVERTY | .128 | .021 | .094 | 6.168 | .000 | |
| PC_RURAL | -3.261E-02 | .003 | -.156 | -10.310 | .000 | |
| TOTAL_NUMB | -.326 | .106 | -.058 | -3.075 | .002 |
a Dependent Variable: PC_BACHDEG
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .821 | .673 | .672 | 5.181 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 142268.529 | 10 | 14226.853 | 529.995 | .000 |
| Residual | 69014.281 | 2571 | 26.843 | |||
| Total | 211282.810 | 2581 |
Race
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 6.850 | .919 | 7.451 | .000 | |
| PERSONS | 3.303E-04 | .000 | 1.957 | 2.401 | .016 | |
| FAMILIES | -1.356E-03 | .000 | -1.923 | -3.206 | .001 | |
| HOUSEHOLDS | 2.781E-05 | .000 | .063 | .094 | .925 | |
| AREALAND | 1.314E-02 | .006 | .045 | 2.212 | .027 | |
| INCOME | 2.014E-04 | .000 | .341 | 9.723 | .000 | |
| PC_OWNER | -.120 | .012 | -.248 | -10.428 | .000 | |
| PC_RURAL | -2.540E-02 | .003 | -.199 | -8.504 | .000 | |
| TOTAL_NUMB | .388 | .099 | .113 | 3.910 | .000 | |
| PC_BACHDEG | -6.664E-02 | .018 | -.109 | -3.610 | .000 | |
| PC_POVERTY | .165 | .019 | .198 | 8.508 | .000 |
a Dependent Variable: PC_MINORIT
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .477 | .228 | .225 | 4.862 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 17947.726 | 10 | 1794.773 | 75.929 | .000 |
| Residual | 60771.641 | 2571 | 23.637 | |||
| Total | 78719.367 | 2581 |
Presence of Manufacturing Activities
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | .888 | .155 | 5.724 | .000 | |
| PERSONS | -1.262E-04 | .000 | -3.082 | -5.493 | .000 | |
| FAMILIES | 2.043E-04 | .000 | 1.194 | 2.882 | .004 | |
| HOUSEHOLDS | 2.811E-04 | .000 | 2.626 | 5.691 | .000 | |
| AREALAND | 4.054E-03 | .001 | .058 | 4.071 | .000 | |
| INCOME | 6.721E-06 | .000 | .047 | 1.899 | .058 | |
| PC_OWNER | -7.945E-03 | .002 | -.068 | -4.044 | .000 | |
| PC_MINORIT | 1.051E-02 | .003 | .043 | 3.180 | .001 | |
| PC_POVERTY | -5.871E-04 | .003 | -.003 | -.178 | .859 | |
| PC_RURAL | -3.450E-03 | .001 | -.112 | -6.827 | .000 | |
| PC_BACHDEG | -9.170E-03 | .003 | -.062 | -2.954 | .003 |
a Dependent Variable: COUNT
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .794 | .630 | .628 | .82 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 2918.980 | 10 | 291.898 | 437.391 | .000 |
| Residual | 1715.786 | 2571 | .667 | |||
| Total | 4634.766 | 2581 |
Presence of Disposal Facilities
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | .168 | .061 | 2.737 | .006 | |
| PERSONS | -4.177E-05 | .000 | -3.414 | -4.596 | .000 | |
| FAMILIES | 1.961E-04 | .000 | 3.835 | 6.990 | .000 | |
| HOUSEHOLDS | 3.870E-06 | .000 | .121 | .198 | .843 | |
| AREALAND | 7.207E-04 | .000 | .034 | 1.829 | .067 | |
| INCOME | 2.370E-06 | .000 | .055 | 1.692 | .091 | |
| PC_OWNER | -2.841E-03 | .001 | -.081 | -3.656 | .000 | |
| PC_MINORIT | 4.729E-03 | .001 | .065 | 3.618 | .000 | |
| PC_POVERTY | 2.669E-03 | .001 | .044 | 2.040 | .041 | |
| PC_RURAL | -1.416E-04 | .000 | -.015 | -.708 | .479 | |
| PC_BACHDEG | -2.087E-03 | .001 | -.047 | -1.699 | .089 |
a Dependent Variable: DISPOSOP
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .593 | .351 | .349 | .3232 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 145.342 | 10 | 14.534 | 139.126 | .000 |
| Residual | 268.588 | 2571 | .104 | |||
| Total | 413.930 | 2581 |
Presence or Manufacturing and Waste Disposal Facilities
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 1.056 | .183 | 5.772 | .000 | |
| PERSONS | -1.679E-04 | .000 | -3.403 | -6.199 | .000 | |
| FAMILIES | 4.004E-04 | .000 | 1.942 | 4.789 | .000 | |
| HOUSEHOLDS | 2.850E-04 | .000 | 2.208 | 4.892 | .000 | |
| AREALAND | 4.775E-03 | .001 | .056 | 4.065 | .000 | |
| INCOME | 9.092E-06 | .000 | .053 | 2.178 | .030 | |
| PC_OWNER | -1.079E-02 | .002 | -.076 | -4.656 | .000 | |
| PC_MINORIT | 1.524E-02 | .004 | .052 | 3.910 | .000 | |
| PC_POVERTY | 2.082E-03 | .004 | .009 | .534 | .593 | |
| PC_RURAL | -3.591E-03 | .001 | -.096 | -6.026 | .000 | |
| PC_BACHDEG | -1.126E-02 | .004 | -.063 | -3.075 | .002 |
a Dependent Variable: TOTAL_NUMB
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .803 | .646 | .644 | .96 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 4346.388 | 10 | 434.639 | 468.228 | .000 |
| Residual | 2386.564 | 2571 | .928 | |||
| Total | 6732.952 | 2581 |
Total Mortality
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 670.995 | 36.014 | 18.632 | .000 | |
| PERSONS | -1.585E-04 | .005 | -.027 | -.030 | .976 | |
| FAMILIES | -1.178E-02 | .016 | -.484 | -.728 | .467 | |
| HOUSEHOLDS | 8.397E-03 | .011 | .551 | .746 | .456 | |
| AREALAND | -1.193 | .229 | -.118 | -5.205 | .000 | |
| INCOME | -1.602E-05 | .001 | -.001 | -.020 | .984 | |
| PC_OWNER | -1.789 | .459 | -.106 | -3.900 | .000 | |
| PC_MINORIT | 1.610 | .753 | .047 | 2.139 | .033 | |
| PC_POVERTY | 2.237 | .766 | .077 | 2.921 | .004 | |
| PC_RURAL | .195 | .117 | .044 | 1.666 | .096 | |
| PC_BACHDEG | -2.992 | .726 | -.140 | -4.123 | .000 | |
| TOTAL_NUMB | -3.536 | 3.792 | -.030 | -.933 | .351 |
a Dependent Variable: AGE_ADJUST
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .273 | .074 | .070 | 185.146 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 6962257.421 | 11 | 632932.493 | 18.464 | .000 |
| Residual | 86760097.312 | 2531 | 34278.980 | |||
| Total | 93722354.733 | 2542 |
Cancer Mortality
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 176.970 | 10.807 | 16.375 | .000 | |
| PERSONS | -2.668E-04 | .002 | -.159 | -.172 | .864 | |
| FAMILIES | 7.473E-05 | .005 | .011 | .016 | .988 | |
| HOUSEHOLDS | 8.259E-04 | .003 | .188 | .248 | .804 | |
| AREALAND | -.398 | .068 | -.135 | -5.820 | .000 | |
| INCOME | 2.963E-04 | .000 | .050 | 1.191 | .234 | |
| PC_OWNER | -.481 | .136 | -.098 | -3.540 | .000 | |
| PC_MINORIT | .326 | .223 | .033 | 1.465 | .143 | |
| PC_POVERTY | .143 | .228 | .017 | .627 | .531 | |
| PC_RURAL | 3.495E-02 | .035 | .027 | 1.011 | .312 | |
| PC_BACHDEG | -.714 | .219 | -.116 | -3.266 | .001 | |
| TOTAL_NUMB | -1.030 | 1.121 | -.030 | -.919 | .358 |
a Dependent Variable: AGE_ADJ_CA
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .198 | .039 | .035 | 54.695 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 307815.911 | 11 | 27983.265 | 9.354 | .000 |
| Residual | 7517660.997 | 2513 | 2991.509 | |||
| Total | 7825476.908 | 2524 |
Low Birth Weight Rates
Coefficients
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |||
| Model | B | Std. Error | Beta | |||
| 1 | (Constant) | 7.558 | .783 | 9.647 | .000 | |
| PERSONS | -1.900E-04 | .000 | -1.557 | -1.706 | .088 | |
| FAMILIES | 5.544E-04 | .000 | 1.087 | 1.617 | .106 | |
| HOUSEHOLDS | 1.615E-04 | .000 | .506 | .675 | .499 | |
| AREALAND | -2.212E-02 | .005 | -.105 | -4.561 | .000 | |
| INCOME | -4.646E-05 | .000 | -.108 | -2.689 | .007 | |
| PC_OWNER | 3.260E-03 | .010 | .009 | .334 | .738 | |
| PC_MINORIT | 7.320E-02 | .016 | .101 | 4.582 | .000 | |
| PC_POVERTY | 7.241E-03 | .016 | .012 | .446 | .656 | |
| PC_RURAL | -4.226E-04 | .002 | -.005 | -.171 | .864 | |
| PC_BACHDEG | -2.789E-02 | .015 | -.063 | -1.835 | .067 | |
| TOTAL_NUMB | -1.064E-02 | .080 | -.004 | -.132 | .895 |
a Dependent Variable: LOW_BIRTH_
Variables Above the double line are controls
Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .209 | .044 | .040 | 3.927 |
ANOVA
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 1799.594 | 11 | 163.599 | 10.607 | .000 |
| Residual | 39363.107 | 2552 | 15.424 | |||
| Total | 41162.702 | 2563 |
Appendix III: Analytical Considerations
One important consideration to our
approach, which we have been unable to resolve at this stage has to do with
the fact that different datasets were derived from different years. Pollution
data comes from EPA datasets for the year 1995. All demographic analysis of
municipalities are from the 1990 census. Health statistics are averaged over
the years 1992-1996. Age adjusted statistics are derived by dividing health
outcome statistics for 18 age categories for the years 1992-1996 by like age
categories of population statistics enumerated in the 1990 census. The reason
for this is that the Pennsylvania Department of Health was unable to provide
us with age group population projections they utilized in their analysis for
all counties and for 25 large municipalities. This means that our municipal
level age adjusted figures differ from the Pennsylvania Department of Public
Health's statistics. That said, we are not at all convinced that state age adjusted
rates are better than our own for this and a number of other reasons discussed
below.
We encountered a number of standardization
problems at the municipal level. Several PA municipalities span county boundaries.
Care must be taken when manipulating and merging datasets. At a basic level,
combining population data with municipal boundary data must take into consideration
the county boundary problem. This problem is further pronounced when one attempts
to combine municipal population, boundary and health data. The Pennsylvania
Department of Public Health does address this problem in some municipalities
by separating health data along county lines. However, in other municipalities
which are split across county lines it appears that the Health Department is
either ignoring health outcome data in one part of the municipality, or aggregating
health outcomes which may occur outside of the county line to the main body
of the municipality, potentially skewing - however slightly - overall county
rates.
In our county level analysis, we utilize Pennsylvania age adjusted cancer death statistics. Elsewhere we utilize our own age adjusted statistics. In both cases, we note additional problems with the data. Municipalities where no health outcome data are reported occur in several different counties. For a number of reasons, we are not sure at all if state health
cover these areas of missing data
by simply omitting outcome data rather than entering 0's for municipalities
where there is no incidence of a particular outcome in a given class. Because
state raw figures and rates appear to be derived by aggregating municipal level
data, this creates a problem which likely becomes more pronounced when age adjusting
health figures are brought into play. If PA health rates at the county level
are based on reported health outcomes aggregated on a per municipality basis
in counties where there are missing data, and the age adjustment process includes
population counts from the 18 age categories used here, then age adjusted rates
in those counties are going to be artificially depressed by using a larger denominator
than is truly warranted.
Overall county by county rates, as well as rates for municipalities with populations over 25,000 people, are reported by the state in their year by year analysis. We aggregated municipal data to produce rates for each county. Our raw rates match the states figures for purposes of developing input files, so our techniques of aggregation and age categorization do not violate any basic ones followed by the state. However, our age adjusted cancer mortality rates differ from the state's figures. We believe our rates differ because our age adjustment procedures utilize 1990 population figures for the age categories where the state utilized population projections note referred to in their book.
Appendix 4: Descriptive
Statistics for Pennsylvania Counties,
and Municipalities and Philadelphia Census Tracts
PA County Health and Demographic Descriptive Statistics
Descriptive Statistics
| N | Minimum | Maximum | Mean | Median | Std. Deviation | |
| Infant Death Rate | 67 | .0 | 13.2 | 6.734 | 6.8 | 2.233 |
| Low Birth Weight Rate | 67 | 4.6 | 11.5 | 6.316 | 6.2 | 1.030 |
| Age Adjusted Total Death Rate | 67 | 430.5 | 689.0 | 497.000 | 486.5 | 40.187 |
| PILCOP Age Adjusted Cancer Death Rate | 67 | 108.6 | 163.9 | 130.472 | 130.1 | 9.989 |
| Age Adusted Non Cancer Death Rate | 67 | 302.2 | 525.1 | 366.528 | 385.1 | 34.579 |
| PERSONS | 67 | 4802 | 1585577 | 177337.96 | 268992.43 | |
| INCOME | 67 | 19170 | 45642 | 26364.60 | 5598.52 | |
| PC_MINORIT | 67 | .6 | 47.9 | 4.290 | 6.464 | |
| PC_POVERTY | 67 | 3.6 | 21.4 | 11.639 | 3.955 | |
| PC_BACHDEG | 67 | 6.7 | 31.9 | 12.669 | 5.250 | |
| Valid N (listwise) | 67 |
PA Municipal Health and Demographic Descriptive Statistics
Descriptive Statistics
| N | Minimum | Maximum | Mean | Median | Std. Deviation | |
| Infant Death Rate | 2561 | .0 | 200.0 | 6.525 | 0 | 12.552 |
| Low Birth Weight Rate | 2565 | .0 | 50.0 | 6.109 | 5.8 | 4.007 |
| Age Adjusted Total Death Rate | 2544 | 55.4 | 4460.7 | 513.759 | 486.4 | 191.988 |
| Age Adjusted Cancer Death Rate | 2526 | 9.9 | 581.9 | 136.879 | 130.1 | 55.670 |
| Age Adjusted Non Cancer Death Rate | 2544 | 26.3 | 4049.0 | 379.530 | 355.5 | 161.079 |
| PERSONS | 2584 | 0 | 1585577 | 4598.16 | 32716.23 | |
| INCOME | 2584 | 0 | 123138 | 27927.60 | 9384.84 | |
| PC_MINORIT | 2584 | .0 | 68.8 | 2.518 | 5.521 | |
| PC_POVERTY | 2584 | .0 | 49.3 | 10.479 | 6.632 | |
| PC_BACHDEG | 2582 | .0 | 67.7 | 11.919 | 9.048 | |
| Valid N (listwise) | 2506 |
Philadelphia Census Tract Health
and Demographic Descriptive Statistics
Descriptive Statistics
| N | Minimum | Maximum | Mean | Median | Std. Deviation | |
| Infant Death Rate | 364 | .0 | 200.0 | 11.798 | 10.1 | 14.459 |
| Low Birth Weight Rate | 364 | .0 | 30.8 | 10.654 | 10.4 | 5.172 |
| Age Adjusted Total Death Rate | 346 | 195.3 | 7577.6 | 771.725 | 710.3 | 468.554 |
| Age Adjusted Cancer Death Rate | 354 | .0 | 2825.9 | 185.304 | 166.1 | 167.483 |
| Age Adjusted Non Cancer Deaths | 346 | 138.2 | 4751.7 | 585.649 | 539.0 | 325.369 |
| PERSONS | 367 | 0 | 17971 | 4320.37 | 2976.46 | |
| INCOME | 353 | 4999 | 150000 | 26174.54 | 13763.79 | |
| PC_MINORIT | 362 | .0 | 100.0 | 46.945 | 39.091 | |
| PC_POVERTY | 362 | .0 | 84.7 | 20.518 | 16.669 | |
| PC_BACHDEG | 359 | .0 | 85.2 | 16.769 | 17.699 | |
| Valid N (listwise) | 345 |
Appendix 5: Glossary of Terms
Poverty Thresholds: 1990
Poverty Thresholds in 1990, by Size of Family and Number of Related Children Under 18 Years
(Dollars)
______________________________________________________________________________________________________________________
| | Related children under 18 years
| Weighted |_______________________________________________________________________
Size of family unit | average | | | | | | | | | Eight
|thresholds| None | One | Two | Three | Four | Five | Six | Seven |or more
___________________________________|__________|_______|_______|_______|_______|_______|_______|_______|_______|_______
One person (unrelated individual)..| $6,652 | | | | | | | | |
Under 65 years...................| 6,800 | 6,800 | | | | | | | |
65 years and over................| 6,268 | 6,268 | | | | | | | |
| | | | | | | | | |
Two persons........................| 8,509 | | | | | | | | |
Householder under 65 years.......| 8,794 | 8,752 | 9,009 | | | | | | |
Householder 65 years and over....| 7,905 | 7,900 | 8,975 | | | | | | |
| | | | | | | | | |
Three persons......................| 10,419 |10,223 |10,520 |10,530 | | | | | |
Four persons.......................| 13,359 |13,481 |13,701 |13,254 |13,301 | | | | |
Five persons.......................| 15,792 |16,257 |16,494 |15,989 |15,598 |15,359 | | | |
Six persons........................| 17,839 |18,693 |18,773 |18,386 |18,015 |17,464 |17,137 | | |
Seven persons......................| 20,241 |21,515 |21,650 |21,187 |20,864 |20,262 |19,561 |18,791 | |
Eight persons......................| 22,582 |24,063 |24,276 |23,839 |23,456 |22,913 |22,223 |21,505 |21,323 |
Nine persons or more...............| 26,848 |28,946 |29,087 |28,700 |28,375 |27,842 |27,108 |26,445 |26,280 |25,268
___________________________________|__________|_______|_______|_______|_______|_______|_______|_______|_______|_______
Source: U.S. Census Bureau, Current
Population Survey.
Income - Average household
income is calculated by totaling income in the area of aggregation divided by
total number of households. Median household income is the amount which divides
the income distribution into two equal groups, half having incomes above the
median, half having incomes below the median. The medians for households, families,
and unrelated individuals are based on all households, families, and unrelated
individuals, respectively. The medians for people are based on people 15 years
old and over with income. We use both average household income and median household
income in this report.
Low Birth Weight Rate - Low
birth weight is a major public health problem in the United States, contributing
substantially both to infant mortality and to childhood handicap. Both low birth
weight (conventionally defined as less than 2,500 grams, or 5 pounds, 8 ounces)
and its major antecedent, preterm delivery (usually referring to birth prior
to 37 completed weeks of gestation), are more common in the United States than
in most other Western European nations, and these differences account for our
nation's relatively poor infant mortality. The principal determinant of low
birth weight in the United States is preterm delivery, a phenomenon of largely
unknown etiology. Preterm delivery is more common in the United States than
in many other industrialized nations, and is the factor most responsible for
the relatively high infant mortality rate in the United States. Although it
is popular to link illicit drug use to low birth weight, a high low birth weight
rate was characteristic of the United States for decades before the cocaine
epidemic of the 1980s. (http://www.futureofchildren.org/LBW/03LBWPAN.htm).
Age Adjusted Mortality Statistics are derived by comparing actual mortality within eighteen specific age categories to expected figures for those categories as provided for in 1940 standard million statistics from the Centers for Disease Control (CDC). Calculations were done using a CDC software package called Health Information Retreival System (HIRS). This program was designed by the National Center for Chronic Disease Prevention and Health Promotion division of Cancer Control and Prevention. Age adjusted statistics are generated for the purpose of comparing unlike areas in terms of their age composition.